Learner credit data, also known as learner completion data or individual credit data, are the records of CME and/or Maintenance of Certification (MOC/CC) credits earned by your physician learners through the completion of an accredited CME activity. Only accredited CME providers are able to upload learner credit data into ACCME’s Program and Activity Reporting System (PARS). For your physician learners, this data includes:
- First and last name
- State medical license ID and/or certifying board ID
- Month and day of birth
Published Date
January 16, 2023
Reporting learner credit data in ACCME’s Program and Activity Reporting System (PARS) is not required. It is an opportunity that has been made available through PARS for all accredited providers so that we can move the system forward to a digitized approach to reporting and managing learner credit data. By entering learner credit data in PARS, you can:
- Decrease physicians’ reporting burden, giving them more time to focus on patient care.
- Reduce your work responding to queries and certificate requests from physicians; PARS can become your system of record for physician credit data, replacing the need to issue paper or e-certificates following completion of activities.
- Reinforce the value of your activities to learners and other stakeholders.
- Support regulatory authorities by providing easier access to verified CME and Maintenance of Certification/Continuous Certification (MOC/CC) credit data. Learner credit data entered in PARS will be made available to the participating state medical licensing boards and certifying boards in collaboration with the ACCME, eliminating the need for physicians to track and submit their credits to these boards manually. For all state licensing boards, physician learners are able to create profiles in CME Passport to view and transmit an official transcript of the CME and MOC/CC credit that has been reported on their behalf.
Published Date
January 16, 2023
By entering learner credit data in PARS, you can:
- Decrease physicians’ reporting burden, giving them more time to focus on patient care.
- Reduce your work responding to queries and certificate requests from physicians; PARS can become your system of record for physician credit data, replacing the need to issue paper or e-certificates following completion of activities.
- Reinforce the value of your activities to learners and other stakeholders.
- Support regulatory authorities by providing easier access to verified CME and Maintenance of Certification/Continuous Certification (MOC/CC) credit data. Learner credit data entered in PARS will be made available to the participating state medical licensing boards and certifying boards in collaboration with the ACCME, eliminating the need for physicians to track and submit their credits to these boards manually. For all state licensing boards, physician learners are able to create profiles in CME Passport to view and transmit an official transcript of the CME and MOC/CC credit that has been reported on their behalf.
Hear more from ACCME’s CEO and President, Graham McMahon, MD, MMSc, on the value of entering learner credit data in PARS here.
Published Date
January 16, 2023
We understand that reporting learner credit data may be a new process for you, and we’re here to help! We hosted a series of webinars to demonstrate how to report learner credit data in ACCME’s Program and Activity Reporting System (PARS) and answer questions about the process. View a recording of the webinar here.
Published Date
January 16, 2023
To delete a learner record through the web interface, you will have to first make sure that the original record has fully processed with an Accepted response. You cannot delete a record with a “Submitted” status. You can hover over the learner’s name to select it for deletion or use the checkmarks next to as many learners as needed to bulk delete.
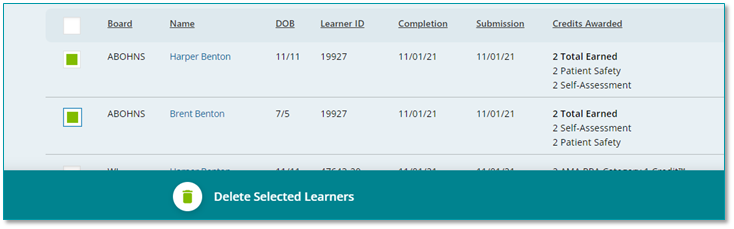
This delete may take up to a few days to fully process with the board, and you will know when it has successfully deleted when the learner record no longer appears in PARS.
You can also delete learners through the batch upload methods or web services. To do this you would indicate a record action of “Delete” in your upload.
Last Revised
November 16, 2021
PARS will send a rejection report when learners are rejected by the board. The email will contain an error message explaining what caused the rejection (for example the learner has already earned the maximum amount of points for the activity). Providers can also see the reason for rejection by hovering over the Rejected status in the PARS interface.
Certain boards (ABA and ABP) will check and enforce granting credit to a diplomate for each unique activity (ACCME Activity ID) once per day (date completed). These implementations are in place to reduce the incidence of accidental duplicate MOC credit reported to the boards with a few exceptions:
- For ABP: This excludes credit for Internet Searching and Learning and Journal-based CME activities. Learners can be reported more than once with the same completion date for this activity type.
- For ABA: If the activity offers both CME and CME which counts for Patient Safety, a max of two participation records for the unique activity be allow diplomate per day – one record including the amount of CME + Patient Safety earned, and (if applicable) one record including the remainder of the CME earned. See the tutorial above for more information regarding multi-credit type reporting.
Yes. Learners can be reported for their engagement in an activity up to the maximum amount available. Learners can be reported in quarter-hour increments (.25) and can be reported within the same activity multiple times depending how/when the credit is earned.
The American Board of Pediatrics (ABP) and American Board of Anesthesiology (ABA) only allow one completion date per activity per learner, so if you need to report a learner multiple times for one of these boards you will need to make sure the completion date is not the same for each of these instances.
You should report learners for MOC credit as they engage in the RSS and complete any evaluation/participation requirements in order to earn MOC credit. You should not wait until the end of the year to report the number of credits earned for an RSS.
In PARS, you can report the completion date as the date of the session attended and award the number of points earned for the session.
Last Revised
November 16, 2021
A participation threshold, or passing standard, clearly communicates to the learner exactly what needs to be done in order to earn MOC credit. This can be set according to the intent of the evaluation and is determined by the provider.
Examples:
- A provider evaluates learners by using case discussions as part of their hospital’s grand rounds. In order to earn MOC credit for the activity, the learners must actively engage in the conversation, and participation is verified by a group leader or observer. The person facilitating this can then attest that the learners have met the participation requirements needed to earn MOC credit.
- If a provider uses a post-test as part of evaluation, the activity planners and/or faculty can determine the minimum number of items that the learners would need to answer correctly to demonstrate that they have adequately absorbed the content of the activity.
When you submit participant completion data, PARS will verify the participant’s information against simple validation rules, and if verified, will transmit the record to the certifying board(s) for further validation. After this has processed, the participant record status will change to “accepted” or “rejected” in PARS. This process typically takes about 24 hours to complete, however this timing can vary. If a learner record is rejected an email notification will be sent to the primary contact listed for your organization, and the reason for rejection will appear in PARS. If you need to change your organization’s primary contact, this can be done by going to your organization’s profile and selecting the “contacts” tab.
If the participant data submitted via PARS does not match the information in a diplomate’s board record, PARS will not be able to confirm the participant’s identity and will not accept the completion record. The provider will be notified immediately via a validation error message in the PARS interface or in the batch upload report, depending on what data submission method is being used. The provider will subsequently need to reach out to the learner to obtain the correct information and re-enter the corrected data for it to be successfully submitted to the certifying board.
Learning from teaching activities are personal learning projects designed and implemented by the learner with facilitation from the accredited provider. This type of activity recognizes the learning that occurs as physicians prepare to teach. Learning from teaching represents a range of activities in which an accredited provider can facilitate practice-based learning and improvement – where the ‘practice’ could be the person’s professional “teaching practice” or “clinical practice” or “research practice.
Examples of learning from teaching activities:
- To prepare for teaching a skills workshop at a surgical specialty society meeting, physician faculty find that they need to learn how to operate a new laparoscopic device that will be used during the workshop. The specialty society, as an accredited provider, facilitates their training on the new device as a learning from teaching activity for the faculty prior to their teaching engagement.
- An accredited provider makes available a learning from teaching activity for new faculty in the form of “individualized learning projects.” In the activity, new faculty assess what knowledge and skills they need to teach more effectively, and then the provider makes available training and feedback to improve the new faculty members’ teaching skills. This includes one-to-one mentorship and training with educational experts.
When you report learning from teaching in PARS, aggregate your data for learning from teaching for all learners into one activity. The number of learners should equal the number of individuals who participated in this activity. The amount of credit may be reported as the maximum amount of credit a learner could earn for a learning from teaching activity.
For example, a provider created a learning from teaching activity for 10 learners. The maximum number of credits a learner could earn over the 12-month period was 10 credits. In PARS, the provider would report this as a learning from teaching activity with 10 learners and 10 credits.
Each learning from teaching activity should be reported for a maximum of a 12-month period. If this activity is available for longer than 12 months, it should be reported as a separate activity each year
Yes, training on broad, cross-specialty topics can be registered for MOC as demonstrated by the professional practice gap(s) and content of the activity and if the provider is meeting all requirements listed in the program guide. Here are some examples:
- Advanced Cardiac Life Support (ACLS)
- Advanced Trauma Life Support (ATLS)
- Clinician Burnout
- Electronic Health Records (EHR)
- Ethics/Professionalist
- Grand Rounds, Tumor Boards, Morbidity and Mortality
- Opioid Education
- Overall Wellness
- Patient Safety
- QI Basics
- Shared Decision-making
- Team-Based Care
These types of activities can also be registered for multiple boards as this content will typically be relevant for multiple specialties.
Yes, activities which are relevant to multiple specialties can be registered for more than one board. Certain activities may be relevant to any specialty.
Yes, you may offer learners the opportunity to earn different types of credits for the same activity as long as the activity meets the different requirements for each available credit type. To determine what specific credit combinations learners may earn for each board and their requirements, please refer to the CME for MOC Program Guide.
The ACCME has created a CME for MOC program guide which details the requirements for offering MOC as part of your organization’s educational program.
This program guide contains an activity planning guide which goes through the requirements step by step to assist you in meeting these criteria when planning and implementing MOC activities. This guide is also available as a stand-alone document for providers to use when planning their CME activities as offering MOC.
Each board has a statement that providers should use in order to inform learners that your activity offers MOC for a specific board (or boards). These statements should be provided to learners on any advertising materials and programs prior to the activity. In general, these statements require that you inform your learners for which board(s) the activity is registered, how many credits they can earn, and for which credit types. Several boards also have CME for MOC badges available for use in your advertisements, however this is optional.
Once an activity is registered in PARS for MOC, the activity will appear in CME Passport for physicians to search and find out more information.
Last Revised
November 16, 2021
Accredited CME providers use PARS to enter and register CME activities that count for MOC. A provider can use PARS to enter in CME activities, and complete a few additional steps in order to register an activity for MOC.
The ACCME has created a step-by-step tutorial which outlines this process in PARS.
Last Revised
November 16, 2021
Accredited providers should report multi-session regularly scheduled series (RSS) as a single activity in PARS, regardless of whether the entire series offers MOC or not. You should not enter individual sessions of the series as separate activity instances in PARS. When completing the fields for MOC in PARS, provide the maximum number of MOC points that are available to the participants for the entire series.
If not all sessions in an RSS offer MOC, report the maximum number of MOC points for the sessions that do meet MOC requirements. For example, if the RSS meets for 1 hour monthly (12 hours total for the year), but only 5 of the sessions offer MOC, you would report 12 hours of instruction/CME for the activity but enter 5 points in the data field asking for the number of MOC points.
Some boards accept AMA credit towards their certification requirements. For these boards the field to enter MOC credit will default to the amount of CME.
Each provider must have systems, resources, and processes in place to:
Collect and report the following data:
- Learner’s certifying board ID number
- First name
- Last name
- Month and day of the date of birth (mm/dd)
- Activity completion date
- Credit type(s) and amount of credit earned
Obtain permission from the learner to share the credit information with their board via ACCME PARS.
Transmit the credit information to ACCME on behalf of the learner in a timely manner. It is the ACCME and the certifying board’s expectation that learners be entered into the system no more than 30 days after the physician has completed the evaluation requirements to earn MOC.
Learner credit data is reported through PARS and can be entered into the system in a variety of ways.
- Entering learners manually in the PARS interface.
- Using the Excel, or XML batch upload method.
- Reporting Learners via ACCME’s web service.
The ACCME has created a step-by-step tutorial that goes into detail for each of these methods.
Last Revised
November 16, 2021
Providers are encouraged to register their activities for MOC as far in advance of the activity start date as possible. This allows learners to find the activity on CME Passport. This also allows providers to enter participant data quickly after the event occurs.
Providers should not wait until the end of the year to report activities registered for MOC; they should enter them into PARS as they are planned prior to advertising these activities as offering MOC to their physician learners.
Users can report learners for different credit amounts within a single record for all entry types.
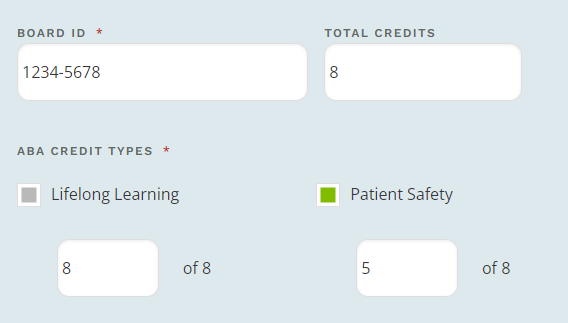
In this example the learner has earned 8 Lifelong Learning credit, 5 of which count towards Patient Safety requirements. The same can be done via Excel batch upload, XML, and web service transactions.
Last Revised
January 16, 2023
No, providers should report any multi-session annual meeting as a single CME activity in PARS. If registering an activity for MOC, you may designate the maximum amount of MOC points offered to reflect only the sessions that offer MOC.
For example, if your annual meeting includes 20 1-hour sessions, but only 5 sessions during that meeting offer MOC, then you should enter 5 points in the data field asking for the number of MOC points.
Some boards accept CME credit towards their certification requirements. For these boards the field to enter MOC credit will default to the amount of CME.
Yes. A provider can select multiple practice areas if the activity covers more than one focused topic. A list of all practice areas can be found in the CME for MOC Program Guide within each board’s section.
These practice areas will appear in CME Passport when the learners search on specific topics.
Last Revised
November 16, 2021
We have collaborated with American Board of Medical Specialties (ABMS) certifying boards to simplify and align the Maintenance of Certification (MOC) process to better meet the needs of physicians and educators. MOC is also referred to as Continuing Certification or Continuous Certification. Although it may be called different names by different boards, the intent is the same. These collaborations increase the number and diversity of accredited CME activities that meet the requirements for MOC and streamline the process for accredited CME providers and physicians.
CME providers do not need to submit MOC applications for approval to the certifying boards that are collaborating with the ACCME. Instead, accredited CME providers use PARS to register activities for these programs using a trust and verify framework. As part of this registration process, providers attest to compliance with certifying board requirements, agree to collect the required individual learner completion data and report it via PARS, agree to abide by certifying board/ACCME requirements for use of the data, agree to allow ACCME to publish data about the activity on ACCME’s website, and agree to comply with requests for information about the activity if the activity is selected for review by the ACCME.
If you are new to MOC, you may want to first read the CME for MOC beginner’s guide, as this goes over the collaboration at a high level.
A provider must first have a mechanism in place to obtain permission from the learner to share the information with the ACCME so that it can be transmitted to their certifying board.
You will need to collect the following information from each board-certified physician claiming MOC in order to report their participant completion data in PARS:
- Date of completion
- Learner’s certifying board ID (optional for ABS)
- First name
- Last name
- Date of birth (month/day only)
This information is used to ensure that the data is accurate and valid, and associated with the correct board-certified physician when it is being reported to the board.
In addition to this collected information, you will need to indicate which activity the learner completed, along with the credit type(s) and how many MOC points were earned.
There are four options available to register a CME activity for MOC in PARS:
- Entering the activity manually in the PARS interface and completing additional fields required to register the activity for MOC.
- Using the Excel batch activity upload method, including the certifying board’s MOC registration data in the file.
- Using the XML batch activity upload method, including the certifying board’s MOC registration data in the file.
- Registering activities via ACCME’s web service, including the certifying board’s MOC registration data in the XML sent.
You cannot batch upload the MOC registration information for activities using the tab-delimited batch upload option. However, if you enter the general information for activities required by PARS via tab-delimited batch upload, the certifying board’s MOC registration fields can then be completed manually in PARS for any activity that you wish to register for MOC.
For more information see Technical Information for Submitting Data via Batch Upload or Web Services.
Last Revised
November 16, 2021
We encourage CME providers to submit participant data as soon as possible after the activity or evaluation component has been completed, so that points earned will reflect in the physician’s records. Accredited providers are asked to submit learner completion data to PARS within 30 days of the learner’s completion of the activity/evaluation.
Please note: Many board-certified physicians need to complete their MOC activities by December 31 in order for the MOC points to count toward any MOC requirements that are due by the end of the year. To that end, providers should report participant completion data by December 31 to ensure that the MOC points count towards this year’s requirements.
ABP diplomates must meet yearly reporting requirements related to completion of activities by December 1. Activities completed after December 1 must have completions entered immediately into PARS.
For activities that span multiple years (such as enduring materials), learner data should be reported in the reporting year the learner participated. Activities should be entered into PARS for each year they are active, and learners reported under the corresponding ACCME Activity ID.
PARS will be open to accept late learner completion data through March 31 two years after the reporting year, after which time that reporting year will be closed for learner completion data. This means that any 2020 learner completion can be entered into PARS for 2020 activities until March 31, 2022. 2021 completions can be entered until March 31, 2023, etc. If you have a learner completion that can no longer be accepted into PARS, please contact the specialty board directly to see if they will accept the credit on their end. Contact information for the boards can be found in the CME for MOC Program Guide in each board’s section.
Learner completion should still be reported in a timely manner after the learner has engaged in the activity, however PARS allows late reporting for exceptions due to technical error or issues with the learner claiming credit.
Your learners should be able to provide you with their certifying board ID number. If they do not know their ID, they can reach out to their specific certifying board to obtain it. Some of the boards have public look-up tools which CME providers can use to find this information as well.
- American Board of Anesthesiology (ABA) diplomates have an eight-digit board ID that begin with the number three (for example, 3555-5555). The board ID is not the same number that is printed on diplomates’ certificates. Diplomates can locate their ID number by logging into their personal ABA portal account.
- American Board of Internal Medicine (ABIM) diplomates have a board ID number that can be up to six digits. This number is printed on diplomates’ certificates. ABIM diplomates can find their board ID by logging into their ABIM Physician Portal or by searching here.
- American Board of Ophthalmology (ABO) diplomates have a board ID number that can be up to five digits. This number is not printed on diplomates’ certificates. Diplomates can locate their ID number by logging into their personal MOC Status Page.
- American Board of Otolaryngology–Head and Neck Surgery (ABOHNS) diplomates have a board ID number that can be up to five digits. ABOHNS diplomates can find their board ID by searching here.
- American Board of Pathology (ABPath) diplomates have an ID number that consists of numbers only with no leading zeros. Diplomates can locate their ID number by logging into their personal account in ABPath’s online platform.
- American Board of Pediatrics (ABP) diplomates have a board ID number that can be up to seven digits. ABP diplomates can find their board ID by searching here.
- American Board of Surgery (ABS) diplomates can locate their board ID by logging into their ABS portal. The ABS ID is optional for learner reporting, but may facilitate a faster learner match.
These resources are outlined in the CME for MOC Program Guide under each board’s section.
Once learner participation has been reported for a MOC activity, you will not be able to delete it. PARS also restricts certain changes from being made after learner participation has been reported.
If you need assistance making changes to your MOC activity, please contact the ACCME at info@accme.org.
Feedback can be provided back to the learner in several ways. Evaluation results (quiz score, reflective statement review, etc.) can be used as feedback. This is best achieved by correcting misconceptions and incorrect responses, showing learners the correct or optimal response, and providing an explanation as to why the correct answer is the best. This can be done live during the activity, or asynchronously. During a live activity, a case discussion where faculty share with learners the appropriateness of the decisions made and the appropriateness of the case outcome is considered acceptable feedback to participants.
The evaluation guide contains different feedback examples that could be provided to learners.
The ACCME has created a list of example evaluation methods providers could choose to use that would meet MOC requirements for the boards. This document contains several different case examples of how reflective statements could be integrated into an activity.
Participating certifying boards and ACCME share the expectation that accredited providers evaluate the impact of their activities on learners’ knowledge, strategies/skills, performance, and/or patient outcomes (Analyzes Change).
The ACCME has a list of example evaluation methods available that would meet MOC requirements for the boards. This list is not a complete list, but intended to show examples of evaluations a provider could choose to implement.
The provider must include an evaluation component that measures learners’ change. Evaluation refers to a question or series of questions or a reflective task that is designed to assess the activity’s goals and purpose. The evaluation should sufficiently address the goals so that a reasonable determination can be made about the learners understanding of the material and the effectiveness of the educational activity.
The accredited provider may choose to evaluate the impact of the activity at the session level or at the activity level. As well, the provider does not need to be limited to a single method of evaluation per activity. Combinations of approaches to evaluation may produce rich information about learner change.
The accredited provider must be able to demonstrate that the learner has participated in/completed the evaluation for the educational activity in order to submit the learner’s participation completion information for the activity. Anonymous learner collection methods, such as an audience response system that is not tied to an individual would not be acceptable as there is no way to demonstrate individual learner completion.